
|
|
Anaplastic carcinoma |
|
General consideration
Anaplastic carcinoma is the most aggressive human malignancy. There is no successful therapy for the disease. Most patients die within a year. The goal of the therapy is to avoid asphyxia of the patient.
Incidence
The reported incidence of anaplastic carcinoma of the thyroid in iodine-sufficient areas was 5-14% of primary malignant tumors, whereas in endemic goiter regions it was much higher, at about 30% until 2000. Nowadays the incidence of anaplastic carcinoma is decreasing which may be caused either by iodine supplementation or the better management of patient with thyroid nodules. It is well-known that most anaplastic carcinomas evolve in goiters known for decades.
Clinical presentation
Anaplastic carcinoma of the thyroid is one of the most aggressive tumors
in humans. It is advantageous if we look on this tumor not as a
histopathological, but as a clinicopathological entity.
The characteristic clinical presentation and the very poor prognosis
are inseparable from the histopathological picture. A knowledge of the
characteristic clinical picture is very important for the cytologist.
The cytological picture is not difficult to interpret if sufficient
material can be gained by aspiration. Most if not all of the patients
die within 1 year after the diagnosis. If a patient survives for longer
than 1 year, the histopathological slides must be reviewed, for a
possible failure of the initial diagnosis must be presumed in
these cases.
The very characteristic clinical picture:
a large, usually very hard and painless goiter develops extremely
rapidly (within 1 to 4 weeks) in a patient over 60 years. There are no
signs of inflammatory reactions. The patients often present with
dyspnea, dysphagia or stridor. Despite the sudden development of the
tumor, many of the patients have only limited fear about their disease.
A similar but less aggressive clinical presentation may be observed in
most cases of MALT-type
malignant lymphoma.
Ultrasonography
Most anaplastic
carcinomas are hypoechogenic and  unilateral.
Necrosis presented as
echonormal irregular areas are frequent findings within the tumors. In
typical case a whole lobe is affected and only small intact parts can
be found at the periphery of the tumor. Cystic degeneration occurs in
around 30-40% of cases but cystic part of the tumor rarely exceeds 5%.
unilateral.
Necrosis presented as
echonormal irregular areas are frequent findings within the tumors. In
typical case a whole lobe is affected and only small intact parts can
be found at the periphery of the tumor. Cystic degeneration occurs in
around 30-40% of cases but cystic part of the tumor rarely exceeds 5%. 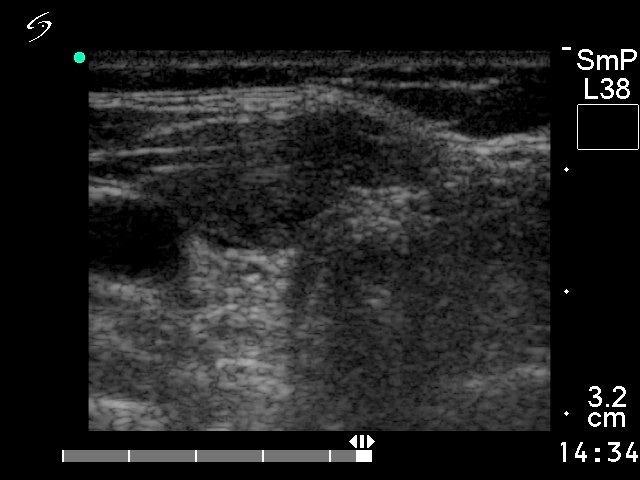 The
vascularization is generally decreased but it has no relevance on
the diagnosis.
The
vascularization is generally decreased but it has no relevance on
the diagnosis.
A direct spread is the
usual growth pattern. The tumor
evolves over
weeks and therefore metastasis is a relatively infrequent phenomenon.
Cytology
If  we
can obtain
adequate material for cytological diagnosis, most of the cases can be
diagnosed cytologically (Us-Krasovec 1996). Highly
atypical, polymorphic tumor cells in a necrotic background occur singly
or may form irregular clusters without any structure; this is the
typical case. Single cell necrosis is a
we
can obtain
adequate material for cytological diagnosis, most of the cases can be
diagnosed cytologically (Us-Krasovec 1996). Highly
atypical, polymorphic tumor cells in a necrotic background occur singly
or may form irregular clusters without any structure; this is the
typical case. Single cell necrosis is a  very rare finding in
thyroid cytology. The only exception
is anaplastic carcinoma.
very rare finding in
thyroid cytology. The only exception
is anaplastic carcinoma.
If there is any doubt, a positive immunocytochemical
reaction for either thyroglobulin or cytokeratin may be used for a
differentiation from malignant lymphoma. From a practical point of
view, the most frequent problem is the difficulty in obtaining
adequate material for cytologic diagnosis. One of the most important
fields in thyroid cytology is the discrimination between thyroid
lymphoma and anaplastic cancer.
Diagnostic problems
1. Clinical picture
- First, it is essential to know exactly whether a large tumor of the neck is thyroidal in origin or not. By means of clinical examination and palpation, it may be very difficult to decide this question in some cases. The possibility of a high-grade malignant lymphoma and a soft tissue tumor of the neck must be ruled out. The thyroid is spared in these cases, which can be proved by US.
- If we know that the painless, very hard, large goiter was developed within a matter of weeks, then in most cases there is no doubt that the patient harbours a malignant tumor of the thyroid. On the other hand, some patients are not aware of the progressivity of their goiter. This is especially important in iodine-deficient areas, where a physician can treat patients with extremely large benign goiters that have developed slowly over decades. Thyroid lymphoma may present in a similar clinical form. It tends to develop somewhat more slowly than anaplastic carcinoma, but the difference is not strict enough for a clear-cut differentiation. However, patients with anaplastic cancer are euthyroid with a normal, or in some cases a suppressed TSH level, while patients with thyroid lymphoma are most often subclinically or clinically hypothyroid (TSH level is elevated). This is explained by the fact that most of the non-Hodgkin's lymphomas of the thyroid are MALT lymphomas that develop in Hashimoto's goiter, a disease which predisposes to hypothyroidism.
- Insular carcinoma of the thyroid has a similar presentation to that of anaplastic cancer, but it tends to develop more slowly, and may occur at a younger age. The cytological picture is strictly different, and is in contrast with the clinical picture and the poor prognosis of insular cancer.
- In many cases of subacute de Quervain's thyroiditis, the patient and the family physician are greatly afraid that the patient is harbouring a malignant tumor. The very typical presentation of subacute thyroiditis differs from that of anaplastic cancer: in the former disease, a severe inflammatory reaction predominates the clinical presentation (i.e. fever, severe pain and an elevated ESR and CRP), a feature lacking in anaplastic cancer.
2. Problems in the cytological interpretation.
-
Obtaining adequate material
As mentioned above, the most important problem is whether sufficient material can be obtained from the
tumor, because
this is a necrotic lesion with extensive degenerative reactions. If the
aspirated material is not suitable for diagnosis, repeat aspirations on
different parts of the tumor are mandatory. In our practice, at least 6
aspirations are performed at the first visit when anaplastic carcinoma
is suspected. In around 30% of our cases, the aspirated material was
inadequate for cytological diagnosis. Six repeat aspirations led to
success in one of these cases. If we cannot obtain enough material even
on repeated aspiration from a very hard, painless, large goiter, then
an iodine-deficient, benign, multinodular goiter, fibrosarcoma and a
rare form of subacute thyroiditis must be ruled out. In the event of
malignant lymphoma, the most important disease to be considered in the
differential diagnostics, the degenerative changes are only limited and
the tumor is very cellular; thus when even repeat aspirations fail to
yield adequate material, the possibility of lymphoma may be ruled out.
the
tumor, because
this is a necrotic lesion with extensive degenerative reactions. If the
aspirated material is not suitable for diagnosis, repeat aspirations on
different parts of the tumor are mandatory. In our practice, at least 6
aspirations are performed at the first visit when anaplastic carcinoma
is suspected. In around 30% of our cases, the aspirated material was
inadequate for cytological diagnosis. Six repeat aspirations led to
success in one of these cases. If we cannot obtain enough material even
on repeated aspiration from a very hard, painless, large goiter, then
an iodine-deficient, benign, multinodular goiter, fibrosarcoma and a
rare form of subacute thyroiditis must be ruled out. In the event of
malignant lymphoma, the most important disease to be considered in the
differential diagnostics, the degenerative changes are only limited and
the tumor is very cellular; thus when even repeat aspirations fail to
yield adequate material, the possibility of lymphoma may be ruled out.
-
Variants of anaplastic cancer
The most important feature is the dominance of dissociated atypical cells, with marked pleomorphism. The cells are irregular in shape, and the cytoplasm is well demarcated. Large tumor cells may frequently be seen. Tumor cells may form multinucleated giant cells. Necrotic
debris and various degenerative changes, including the
presence of histiocytes, lymphocytes and fibroblasts, may be noted.
Irregular sheets of various sizes also occur in the smears. The lack of
any structure of the single cells and clusters is impressive. There is
no other disease with this phenomenon. Well-preserved cells forming
regular groups are rarely seen.
Necrotic
debris and various degenerative changes, including the
presence of histiocytes, lymphocytes and fibroblasts, may be noted.
Irregular sheets of various sizes also occur in the smears. The lack of
any structure of the single cells and clusters is impressive. There is
no other disease with this phenomenon. Well-preserved cells forming
regular groups are rarely seen.
The dominant cell type allows a discrimination of various forms of the disease. Two of these variants are of practical relevance. If elongated cells mimicking atypical fibroblasts predominate, then the possibility of fibrosarcoma must be born in mind. In our practice, only one case of fibrosarcoma has occurred to date. We performed repeat aspirations, but all of the smears were acellular. The patient's history was more indolent than in cases of anaplastic cancer: an extremely hard, large uninodular goiter had developed over 2 years. The small cell variant of anaplastic cancer was a frequent diagnosis more than 20 years ago. Most of these cases were really non-Hodgkin's malignant lymphomas. On the basis of immunohistochemical studies, even the existence of the small cell variant of anaplastic thyroid cancer was questioned. There are articles which provide convincing evidence of the true existence of this tumor type. However, it is probably a very rare tumor with limited practical relevance. (If we give a false cytological report of lymphoma, then as a rule the patient participates either in immunocytochemical examinations or in biopsy of the thyroid. The diagnosis of thyroid lymphoma is no longer accepted without immunohistochemical studies.) Theoretically, small cell variant of anaplastic cancer can be diagnosed at the latest at the stage of histopathological examination of the excised material.
3. Differential diagnostics involving possibilities other than thyroid lymphoma
We discuss here those cases where adequate material can be obtained. This might seem a very important field in thyroid cytology, but in practice it is of only limited relevance, because the clinical picture of anaplastic cancer is so impressive and characteristic. As mentioned earlier, it is essential to be aware of the clinical presentation if the aspiration is not performed by the cytopathologist.
-
Medullary or anaplastic carcinoma?
Among thyroid tumors, medullary carcinoma is the primary differential consideration (Martinelli 1983 , Kini 1984 , Us-Krasovec 1996). This is true for the microscopic analysis, but when the clinical presentation is also taken into account, the problem is not the most important one. In cases involving doubt, serum calcitonin determination should be performed.
-
Fibrosarcoma or anaplastic cancer?
Elongated atypical cells may be seen in both cases. On the other hand, the polymorphism of the tumor cells is not typical in fibrosarcoma. Necrosis is seen only infrequently in fibrosarcoma, whereas this feature is very common in anaplastic carcinoma. Moreover, fibrosarcoma of the thyroid is a rare disease, which develops over a period of years.
-
Well-differentiated carcinoma or anaplastic carcinoma?
Well differentiated carcinoma of the thyroid and atypical adenoma may contain highly atypical cells. In most of the cases, the atypia means the enlargement and the oval character of the cells. However, the disarrangement and irregular shape of the cells that are seen in anaplastic cancer cannot be observed in well-differentiated carcinoma. Even more important difference arise in the clinical presentation, as concerns the age of the patient, the progressivity of the disease, the degree of the enlargement, and the consistency of the thyroid. The clinical picture observed in anaplastic cancer cases is highly specific. In cases with a relatively benign cytological picture corresponding to any type of well-differentiated carcinomas of the thyroid, but with a clinical presentation of anaplastic cancer it must be supposed either that the tumor has an anaplastic component or the tumor is a poorly-differentiated cancer of the thyroid. It is well known that, in most if not all cases of anaplastic cancer, an anaplastic transformation of well-differentiated carcinoma occurs.
- Metastatic carcinoma or anaplastic carcinoma?
Metastatic cancers may contain highly atypical cells resembling those in anaplastic cancer. The cytological picture alone is not sufficient to allow a differentiation between these entities is some cases. A thyroglobuline immunocytochemical reaction is then proposed, but if positive reference cells are not available, a negative thyroglobulin reaction cannot be decisive. Another opportunity is the determination of thyroglobulin in wash-out of the needle. Otherwise the clinical picture is again of decisive help: patients with a secondary carcinoma of the thyroid present with an indolent clinical picture: a slowly-growing, well circumscribed, solitary nodule.
-
The thyroglobulin immuncytochemical reaction in anaplastic cancer
This would be of great importance in problematic cases. However, the reported frequency of a positive reaction for thyroglobulin varies 0% to 70%, with an average of around 20-25% (Kini 1984, De Micco 1987, Hurliman 1987, Shvero 1988). More promising results have been reported from the use of antikeratin, antifat globule membrane antigen and lactoferrin in order to demonstrate the epithelial origin of the tumor (Harliman 1987). The greatest problem is to obtain well-preserved tumor cells from anaplastic cancer for immunocytochemistry.
4. Differential diagnostics - MALT-type thyroid lymphoma
MALT-type thyroid lymphoma is the only disease which presents a similar clinical picture. It evolves more slowly but the difference within weeks in the case of anaplastic carcinoma and within a few months in the case of lymphoma is not enough for a decisive differentiation. Similarly, the difference in palpation is not an impressive difference, a stone hard, and very hard, anaplastic cancer and lymphoma, respectively. In contrast with the similar clinical presentation there is a very strike difference both in further diagnostic steps and therapy and in prognosis. Therefore it is essential to differentiate the two entities in order to avoid unnecessary radicalism in surgery and to avoid delay in adequate chemotherapy in the case of lymphoma.
If we gain
adequate material the
cytological pattern is decisive. Thyroid lymphomas present in most if
not all cases a very cellular picture with a relatively monomorphous
pattern of medium-sized lymphocytes. It strikingly differs from the
presentation of anaplastic carcinomas with isolated highly atypical,
pleomorphic tumor cells.
If we repeatedly cannot gain material enough for cytodiagnosis it is
itself a very strong argument against a MALT-type lymphoma.